

Abstract
<Introduction> Hepatitis B virus (HBV) surface antigen (HBsAg)-positive patients treated with anti-B-cell lymphoma therapy are at high risk of HBV reactivation; indeed, the incidence is as high as 60-80% without antiviral prophylaxis. Hepatitis caused by HBV reactivation usually leads to discontinuation of chemotherapy, which in itself may be fatal. Therefore, several guidelines recommend antiviral prophylaxis for HBsAg-positive patients treated with chemotherapy. However, there is limited evidence regarding the clinical impact of antiviral prophylaxis on HBV reactivation and subsequent hepatitis and long-term outcome, particularly in patients treated with rituximab (R)-containing regimens. To answer these questions, we conducted a nationwide multicenter retrospective analysis for HBsAg-positive patients with diffuse large B-cell lymphoma (DLBCL) treated with R-chemotherapy.
<Methods> Data were collected from HBsAg-positive patients with DLBCL who received R-CHOP or R-THP-COP regimens as an initial chemotherapy (regardless of steroid use) at 29 participating institutions between January 2004 and December 2014. Key exclusion criteria were as follows: seropositive for HCV or HIV; alanine transaminase (ALT) levels ≥ 100 U/L at the time of diagnosis; and a history of decompensated cirrhosis or hepatocellular carcinoma. Medical data were also obtained for HBsAg-negative DLBCL patients (controls), regardless of anti-HBc or anti-HBs seropositivity; these patients were diagnosed within 2 month (before and after 1 month) of the diagnosis date of each HBsAg-positive patient. Hepatitis was defined as an absolute serum ALT level of ≥ 100 U/L. HBV reactivation-related hepatitis was defined as hepatitis accompanied by an absolute serum HBV DNA level of ≥ 3.3 Log IU/mL or an absolute increase of ≥ 2 Log compared with the baseline value. Statistical analysis was performed at the Japanese Data Center for Hematopoietic Cell Transplantation using Stata software Version 13.1 and EZR 1.35. The study was registered at UMIN (ID: 000025574).
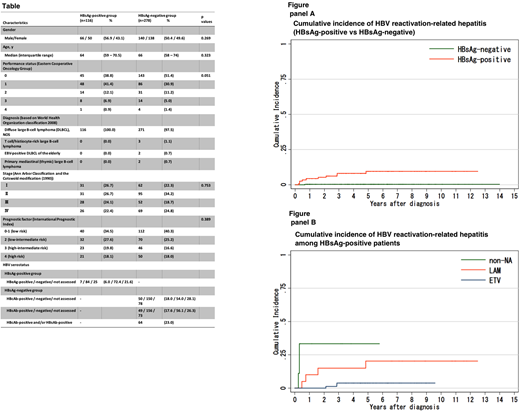
<Results> A total of 394 patients were eligible: 116 (29.4%) were HBsAg-positive and 278 (70.6%) were HBsAg-negative. The baseline characteristics of the two cohorts were similar; exceptions was HBV status (Table). R-CHOP was the most common regimen (n=337, 85.5%), followed by R-THP-COP (n=57, 14.5%). For HBsAg-positive patients with detectable and quantifiable HBV DNA (n=65, 56.0%), the median baseline HBV DNA level was 2.9 Log IU/mL (interquartile range, 2.0-3.7). HBsAg-positive patients were divided into three groups based on prophylactic nucleoside analogue (NA) therapy: no prophylactic therapy (non-NA, n=9), prophylactic therapy with lamivudine (LAM, n=20), and prophylactic therapy with entecavir (ETV, n=87). Of the HBsAg-negative patients, 64 (23.0%) were seropositive for anti-HBc or anti-HBs. The median follow-up time for HBsAg-positive and HBsAg-negative patients was 4.3 years and 4.5 years, respectively. The 4-year cumulative incidence of hepatitis in HBsAg-positive and HBsAg-negative patients was 21.1% (95% confidence interval (CI): 14.1-28.9%) and 14.6% (95% CI: 10.7-19.2%), respectively (p=0.081). Importantly, the 4-year cumulative incidence of HBV reactivation-related hepatitis was higher in HBsAg-positive patients than in HBsAg-negative patients (8.0% (95% CI: 3.9-14.0%) vs. 0.4% (95% CI: 0.0-2.0%, respectively; p<0.001; Figure, panel A). Among HBsAg-positive patients, the 4-year cumulative incidence of HBV reactivation-related hepatitis was highest in the non-NA group (33.3%, 95% CI: 7.8-62.3%), followed by the LAM (15.0%, 95% CI: 3.7-33.5%) and ETV (3.8%, 95% CI: 1.0-9.8%) groups (p<0.001) (Figure, panel B). Remarkably, the 4-year cumulative incidence of HBV reactivation-related fulminant hepatitis was 11.1% in the non-NA group; this was higher than in the LAM (5.0%) and ETV (0.0%) groups (p=0.025). Finally, three non-NA patients (33%) and one LAM patient (5%) (but no ETV patient) died due to HBV reactivation-related hepatitis.
<Conclusions> Prophylactic use of entecavir reduced the incidence of HBV reactivation-related hepatitis and reduced mortality associated with HBV reactivation-related hepatitis in HBsAg-positive patients with DLBCL treated with R-chemotherapy.
Maruyama:Abbvie: Research Funding; Nippon Boehringer Ingelheim: Research Funding; Pfizer: Research Funding; Amgen Astellas BioPharma: Research Funding; Kyowa Hakko Kirin: Honoraria, Research Funding; Celgene: Honoraria, Research Funding; Fujifilm: Honoraria, Research Funding; MSD: Honoraria, Research Funding; Novartis: Research Funding; GlaxoSmithKline: Research Funding; Chugai Pharma: Honoraria, Research Funding; Bristol-Myers Squibb: Honoraria; Takeda: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Eisai: Honoraria, Research Funding; Biomedis International: Honoraria, Research Funding; Solasia Pharma: Research Funding; AstraZeneca: Research Funding; Asahi Kasei Pharma: Honoraria; Dai-Nippon-Sumitomo: Honoraria; Zenyaku Kogyo: Honoraria, Research Funding; Mundipharma International: Honoraria, Research Funding; Ono Pharmaceutical: Honoraria, Research Funding; Astellas Pharma: Research Funding; Otsuka: Research Funding; Dai-ichi-Sankyo: Honoraria. Yamamoto:Bristol-Myers Squibb: Honoraria. Igarashi:Eisai Co Ltd.: Research Funding; Celltrion Inc.: Research Funding; Zenyaku-Kogyo Co.Ltd.: Research Funding; Sanofi K.K.: Research Funding. Izutsu:Takeda: Honoraria, Research Funding; Zenyaku: Research Funding; Amgen: Research Funding; Gilead Sciences: Honoraria; Solasia: Research Funding; Sanofi: Research Funding; Otsuka: Honoraria; Mundhi: Honoraria; Kyowa Hakko Kirin: Honoraria; Abbvie: Honoraria, Research Funding; Bayer: Consultancy, Honoraria, Research Funding; Symbio: Research Funding; Celltrion: Research Funding; Chugai: Honoraria, Research Funding; Nihon Medi-Physics: Honoraria; MSD: Honoraria; Celgene: Consultancy, Research Funding; Bristol- Myers Squibb: Honoraria; Daiichi Sankyo: Honoraria, Research Funding; Astellas: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; HUYA Bioscience International: Research Funding; Eisai: Honoraria, Research Funding; Novartis: Honoraria; Ono: Honoraria, Research Funding; Meiji Seika: Honoraria; Shionogi: Honoraria; Asahi Kasei: Honoraria. Uchida:Nippon Shinyaku: Honoraria; Pfizer: Honoraria; Bristol-Myers Squibb: Honoraria; Meiji Seika Pharma: Honoraria; Mundipharma: Honoraria; Celgene: Honoraria; Teijin: Honoraria; Novartis: Honoraria; Janssen Pharma: Honoraria; Takeda Pharmaceutical: Honoraria; Otsuka Pharmaceutical: Honoraria; Eisai: Honoraria; Kyowa Hakko Kirin: Honoraria; Chugai Pharmaceutical: Honoraria. Tsukamoto:Chugai: Research Funding; Eisai: Research Funding; Pfizer: Research Funding; Kyowa-Kirin: Research Funding. Nosaka:Celgene Co. LTD.,: Honoraria; Chugai Pharmaceutical Co.LTD.,: Honoraria; Kyowa Kirin Pharmaceutical Development, Inc.,: Honoraria; Eisai Co. Ltd.,: Honoraria; Ono Pharmaceutical Co.LTD.: Honoraria; Bristol-Myers Squibb: Honoraria. Ueda:Rikaken Co. Ltd.: Research Funding; Medical and Biological laboratories Co. Ltd.: Research Funding; Chugai Pharmaceutical Co. Ltd.: Research Funding; Kyowa Hakko Kirin Co. Ltd.: Honoraria, Research Funding; Terumo Co.: Consultancy; Ono Pharmaceutical Co.: Consultancy, Honoraria, Research Funding; Mundipharma K.K.: Consultancy. Mizokami:Sysmex Corporation: Honoraria; Gilead Sciences: Honoraria. Kusumoto:Bristol-Myers Squibb: Honoraria, Research Funding; Chugai Pharmaceutical Co. Ltd: Honoraria, Research Funding; Kyowa Hakko Kirin: Honoraria, Research Funding.

